

The Deadly Effects of Fructose
Why Fructose is so toxic

In 2009, Dr. Robert Lustig, a pediatric endocrinologist at the University of California, San Francisco delivered a ninety minute lecture entitled “Sugar: The Bitter Truth”. It was posted on YouTube as part of the university’s medical education series. Then a funny thing happened. It went viral.
It was not a humorous cat video. It was not a video of a toddler throwing a baseball into Dad’s groin. It was a nutrition lecture filled with biochemistry and complicated graphs. But there was something about this particular lecture that grabbed the world’s attention and refused to let go. It has now been viewed more than six million times. What was this attention-grabbing message? Sugar is toxic.
Sucrose, against all logic and common sense, had not always been considered unhealthy. The U.S. Food and Drug Administration undertook a comprehensive review in 1986, eventually declaring “there is no conclusive evidence on sugars that demonstrates a hazard.” Even as recently as 2014, the American Diabetes Association website stated “experts agree that you can substitute small amounts of sugar for other carbohydrate-containing foods into your meal plan.”
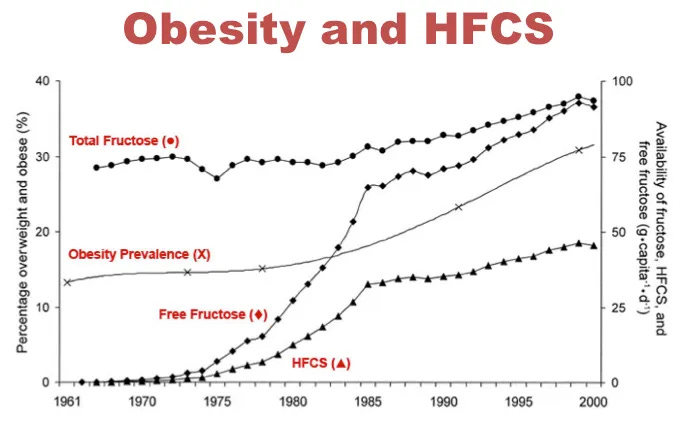
The tide began to turn in 2004 when Dr. George Bray from the Pennington Biomedical Research Center of Louisiana State University showed that the increase in obesity closely mirrored the increased use of high-fructose corn syrup in the American diet. In the public consciousness, high-fructose corn syrup developed as a major health issue. Others correctly pointed out that high-fructose corn syrup use increased in proportion to the decreased use of sucrose. The rise in obesity really mirrored the increase in total fructose consumption, whether the fructose came from sucrose or from corn syrup.
Dr. Lustig was not the first physician to warn about the dangers of eating too much sugar. In 1957, prominent British nutritionist Dr. John Yudkin warned anybody who would listen about the danger. Faced with the growing incidence of heart disease, Yudkin recognized that sugar likely played a prominent role. However, the world instead chose to follow Dr. Ancel Key’s condemnation of dietary fat instead. Sugar’s main danger, other than the increased calories, was dental cavities. After leaving academic medicine, Yudkin wrote an eerily prescient book entitled “Pure, White and Deadly”, but his warnings have largely been unheeded.
The 1977 Dietary Guidelines for Americans distinctly warned the general public about the dangers of excessive dietary sugar, but this message got lost in the anti-fat hysteria that followed. Dietary fat was public enemy number one, and concerns about excess sugar faded like the last rays of sunset. Sugar consumption rose steadily from 1977 to 2000, paralleled by the rising obesity rates. Ten years later, type 2 diabetes followed doggedly like a bratty little brother.
Obesity alone, however cannot explain the entire upsurge in diabetes. Many obese people have no evidence of insulin resistance, diabetes or metabolic syndrome. On the other hand, there are also the skinny type 2 diabetics. This is obvious on a national level, too. Some countries with low obesity rates have high diabetes rates while the opposite is true, too. Sri Lanka’s obesity rates have remained at 0.1% from year 2000–2010 while diabetes rose from 3% to 11%. Meanwhile, over the same time period, in New Zealand, obesity rose from 23% to 34% while diabetes fell from 8% to 5%. Sugar consumption may well explain much of this discrepancy.
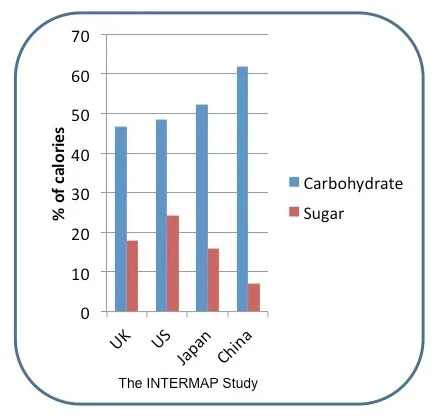
What was it specifically about sugar that makes it particularly toxic? It isn’t simply that sugar is a highly refined carbohydrate. The Chinese diet of the early 1990s, as documented by the INTERMAP study, was based primarily upon white rice and therefore very high in refined carbohydrates. This presents an apparent paradox, since they suffered little obesity or type 2 diabetes.One crucial point is that the 1990s Chinese diet was extremely low in sugar. Most refined carbohydrates such as white rice, are composed of long chains of glucose, whereas table sugar contains equal parts glucose and fructose. As Chinese sugar consumption started to increase in the late 1990s, diabetes rates moved in lockstep. Combined with their original high carbohydrate intake, this is a recipe for the diabetes disaster.
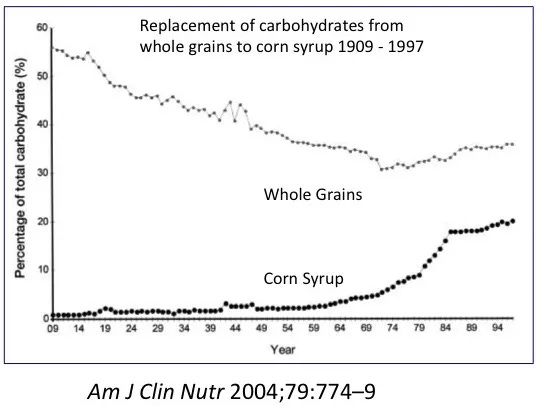
To a lesser extent, the same story played out in the United States as well. Carbohydrate consumption gradually switched from grains to sugar in the form of corn syrup. This paralleled the rising incidence of type 2 diabetes.
When data from over 175 nations is reviewed, sugar intake is intricately linked to diabetes even independent of obesity. For example, Asian sugar consumption is rising at almost 5 percent per year, even as it has stabilized or fallen in North America. The result has been a made-in-China tsunami of diabetes. In 2013, an estimated 11.6 percent of Chinese adults have type 2 diabetes, eclipsing even the long-time champion: the U.S., at 11.3 percent. Since 2007, 22 million Chinese were newly diagnosed with diabetes — a number close to the population of Australia.
Things are even more shocking when you consider that only 1 percent of Chinese had type 2 diabetes in 1980. In a single generation, the diabetes rate rose by a horrifying 1160 percent. Sugar, more than any other refined carbohydrate, seems to be particularly fattening and leads specifically to type 2 diabetes. Yet the Chinese were being diagnosed with diabetes with an average body mass index of only 23.7, which is considered in the ideal range. By contrast, American diabetics averaged a BMI of 28.7, well within the overweight category.
The prevalence of diabetes climbs 1.1 percent for every extra 150 calories per person per day of sugar. No other food group showed any significant relationship to diabetes. Diabetes only correlates with sugar, not other sources of calories.
Similar data can be found for sugar-sweetened beverages, one of the largest sources of sugar in the American diet. Between the late 1970s and 2006, the per capita intake of SSBs almost doubled to 141.7 kcal/day. Each additional 12-oz serving of SSB increases the risk of diabetes by 25%. Risk of metabolic syndrome is increased by 20%.
High fructose corn syrup consumption, chemically almost identical to sugar also shows a tight correlation to diabetes. Countries using large amounts of HFCS suffered a twenty percent increased prevalence of diabetes compared to those that did not. The United States, by the way is the undisputed heavyweight champion of HFCS with a per capita consumption of almost 55 pounds.
What distinguishes sugar from other carbohydrates? What is the common link to disease? Fructose.
Fructose
Paracelsus (1493–1541), the Swiss-German physician considered the founder of modern toxicology neatly summarized one of its most basic principles as “The dose makes the poison”. Anything, even if typically consider beneficial, can be harmful in excessive amounts. Oxygen can be toxic at high levels. Water can be toxic at high levels. Fructose is no different.
Natural fruit consumption contributes only small amounts of fructose to our diet, in the range of 15 to 20 grams per day before the year 1900. By World War II, the increased availability of sugar allowed yearly per capita consumption of 24 g/day. It rose steadily to 37 g/day by 1977.
The development of high-fructose corn syrup allowed fructose intake to skyrocket to 55 g/day in 1994 accounting for 10% of calories. Consumption peaked in the year 2000 at 9 percent of total calories. Within the space of 100 years, fructose consumption had increased by five fold. Adolescents in particular were heavy users of fructose often eating as much as 25% of their calories as added sugars at 72.8 grams/day. Currently, it is estimated that Americans eat 156 pounds of fructose-based sweeteners per year. The dose makes the poison.
High-fructose corn syrup was developed in the 1960s as a liquid-sugar equivalent of sucrose. Sucrose was processed from sugar cane and sugar beets. While not exactly expensive, it wasn’t exactly cheap. High-fructose corn syrup, however, could be processed from the river of cheap corn that was flowing out of the American Midwest — and that was the decisive factor in favor of high-fructose corn syrup. It was cheap.
Soon, high-fructose corn syrup found its way into almost every processed food imaginable. Pizza sauce, soups, breads, cookies, cakes, ketchup, sauces — you name it, it probably contained high-fructose corn syrup. It was cheap, and big food companies cared about that more than anything else in the world. They raced to use high-fructose corn syrup at every opportunity, often replacing sucrose due to its cost advantage.
Sugar basics
Glucose is the main sugar that is found in the blood. The terms “blood sugar” and “blood glucose” are used interchangeably. Glucose can be used by virtually every cell in the body, and circulates freely throughout the body. In the brain, it is the preferred energy source. Muscle cells will greedily import glucose from the blood for a quick energy boost. Certain cells, such as red blood cells, can only use glucose for energy. Glucose can be stored in the body in various forms, such as glycogen in the liver. If glucose stores run low, the liver can make new glucose via the gluconeogenesis process.
Fructose is the sugar found naturally in fruit and the sweetest tasting naturally occurring carbohydrate. Only the liver can metabolize fructose and it does not circulate freely in the blood. The brain, muscles and most other tissues cannot use fructose directly. Eating fructose does not appreciably change the blood glucose level, since they are different sugar molecules.
Table sugar, known as sucrose, is composed of one molecule of glucose linked to one molecule of fructose, making it fifty percent glucose and fifty percent fructose. Chemically, high-fructose corn syrup is composed of fifty-five percent fructose and forty-five percent glucose. Pure fructose is generally not consumed directly, although is can be found as an ingredient in some processed foods.
Carbohydrates are single sugars or chains of sugars all linked together. Glucose and fructose are examples of single sugar carbohydrates. Sucrose is a two-chain carbohydrate since it contains one molecule each of glucose and fructose.
Starches, the main carbohydrate in potatoes, wheat, corn and rice, are long chains of glucose. Produced by plants, starch functions mostly as a store of energy. Sometimes they are stored underground, as in root vegetables, and other times above ground as in corn and wheat. By weight, starch is approximately 70% amylopectin and 30% amylose. Animals, including humans, link glucose together in chains for storage in the form of glycogen instead.
Once eaten, the chains of glucose in starches are rapidly broken down into individual glucose molecules and absorbed into the intestines. The Glycemic Index measures the blood glucose raising ability of various carbohydrates. Pure glucose will obviously cause the largest rise in blood glucose and is therefore given the maximal value of 100. All other foods are measured against this yardstick. Bread, made predominantly of white flour also has an extremely high glycemic index since the refined starch from wheat is quickly digested into glucose.
Other dietary sugars, like fructose or lactose (the sugar found in milk) do not raise blood glucose levels appreciably, and therefore have correspondingly low glycemic index values. Since sucrose is half glucose and half fructose, it has an intermediate glycemic index. Only the glucose portion of sucrose raises blood glucose appreciably.
Fructose, which neither raises blood glucose nor insulin was considered more benign than other sweeteners for many years. An all-natural sweetener found in fruit that didn’t raise the Glycemic Index sure sounded healthy. But it had a hidden dark side, one that was not obvious for many decades.
The toxicity of fructose could not be seen by looking at the blood sugars, only by looking at the slow accumulation of fat in the liver. The key was the fatty liver.
Jason, I have followed you for years and participated in your intermittent fasting groups but your dismissal of supplements is mis-guided, in my opinion. Dr. Justus R Hope and Dr. Paul Marik have done tremendous research on re-purposed drugs and supplements for treating cancer. I hope you will check this out. https://open.substack.com/pub/justusrhope/p/the-daily-pills-that-stop-cancer?r=onxbd&utm_medium=ios
Does that mean fruit is not healthy to eat?