Hacking The Incretin Hormones
How Ozempic works


What are Incretins and Why do We Care?
The GLP-1 agonist drugs, Ozempic and Mounjaro cause significant and sustained weight loss by affecting the incretin hormones. (See my article — What Ozempic teaches us about Weight Loss) So understanding these systems and what foods affect them can lead us to rational food choices to maximize weight Incretins are hormones secreted in the intestines which play several major roles in food intake:
1. Increases insulin secretion in the pancreas to aid digestion
2. Increase satiation — tells us to stop eating
3. Increase satiety — tells us how long before we should eat again
When we eat, the body both digests this food for nourishment, but also secretes hormones to tell us to stop eating. This is a homeostatic mechanism which helps maintain body weight in the ideal range. In the wild, being overweight is a major disadvantage — you can’t catch smaller, faster animals and are more likely to be caught yourself. This is why you never see morbidly obese animals in the natural world, and why almost all animals, including humans have evolved mechanisms to maintain their body fat within a target range.
Understanding the mechanisms and hormones that tell us to stop eating is obviously a major advantage for weight loss. When we feel full, we don’t want to eat, and that causes us to lose weight. Weight loss is about controlling the hunger, rather than controlling the calories (see article — The Roots of the Obesity Epidemic). Obesity is a hormonal imbalance, not a caloric one. Therefore, we must strive to fix the hormones, not the calories. The interest in incretins has exploded as drugs that target the incretins can cause significant and sustained weight loss.
But what are the natural factors that increase incretin release? This is the focus of this article.
There are two main incretins:
1. Glucagon-Like Peptide 1 (GLP1)
2. Glucose Dependent Insulinotropic Polypeptide (GIP)
Incretins are released by different specialized cells in the gut. GLP1 is produced by the L cells in the large and small intestines and are most dense in the ileum (the last part of the small intestine). GIP is produced by the K cells in the duodenum and upper jejenum (the upper parts of the small intestine). Incretins are released in response to nutrients — carbohydrates, lipids and proteins. Incretins are released a few minutes into nutrient intake and peaking about an hour after. What do the incretins do? We know that drugs that increase GLP1 can severely suppress appetite and cause weight loss.
Actions of Incretins
Pancreas
The incretins help digestion by increasing insulin secretion in the pancreas, which tells our bodies to store food energy (as body fat). Hey wait, won’t increasing insulin tend to increase weight? Absolutely. But, doesn’t increasing incretins help weight loss? Absolutely. So what gives? Acutely, right after a meal, insulin increases, but incretins also make us feel full for longer. This reduces overall food intake, and the overall effect is to reduce insulin — in the case of Ozempic, by a lot.
The GLP1 drugs reduce the net area under the curve (AUC), which reflects the total action of insulin over time by almost 50%. Because you eat less, which will increase the amount of insulin released per unit food, but you’ll be eating so much less food that the overall insulin levels are significantly reduced. And lower insulin levels generally cause lower body fat. Less insulin, lower body fat. See my video ‘Why do we get Fat’ for more details.
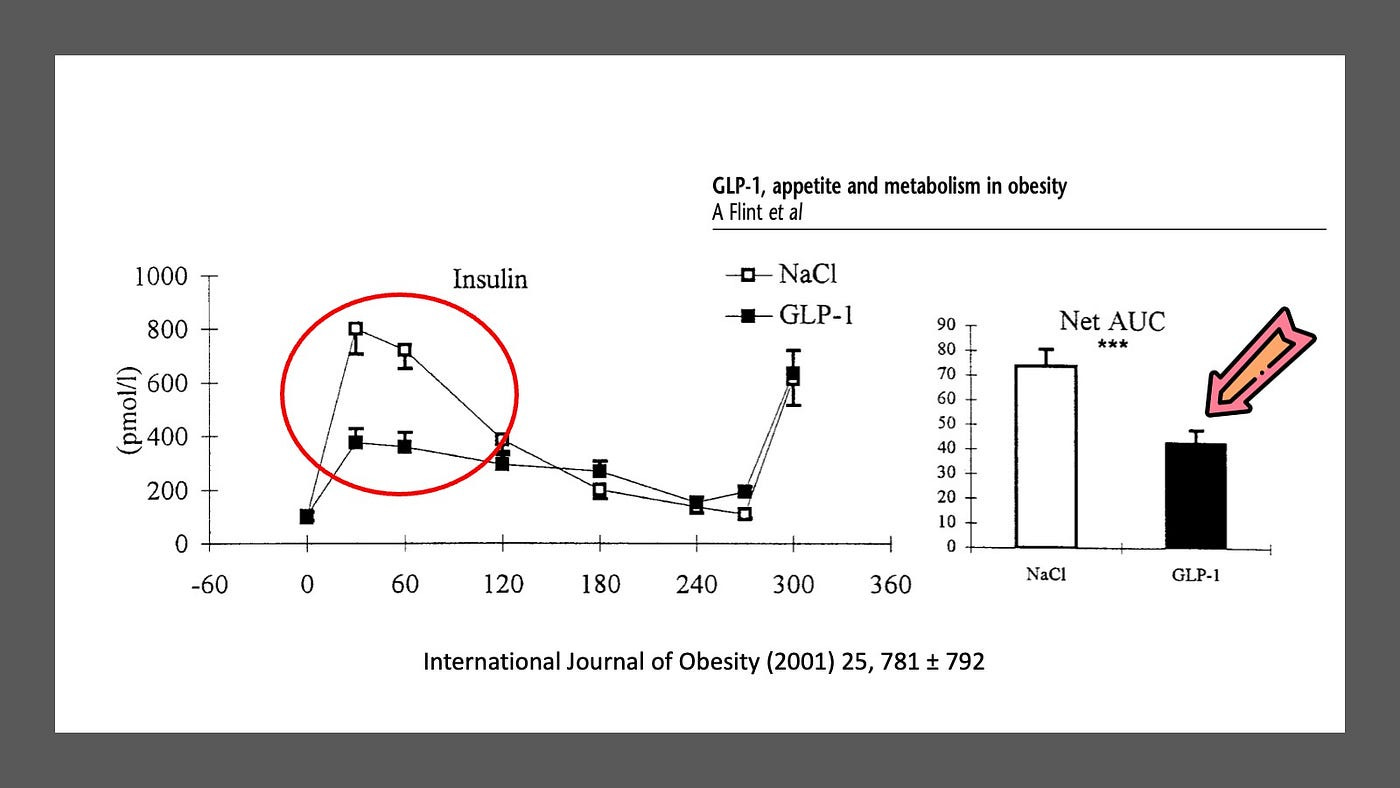
GLP1 drugs significantly reduce overall insulin secretion
Gut Motility
The stomach begins the digestion process by mechanically mixing food with stomach acid. It holds the food, releasing it slowly over time into the small intestines (duodenum). This gives the small intestines time to digest and absorb the nutrients without getting overloaded. GLP1 slows gastric emptying significantly. Slowing the stomach’s release of food slows delayed nutrient absorption and therefore causes a flatter rises in blood glucose (and insulin) after meals.
Stretch receptors in the stomach wall are present to tell us to stop eating. If the stomach is full of food, we need to know this so that we can stop putting more food in. Since the stomach acts as a reservoir for food to be digested, slowing gastric emptying will activate those stretch receptors for longer.
Normally, by the time the food reaches the end of the small intestines, most nutrients should have been absorbed into the body. However, in some cases, there are still unabsorbed nutrients by the end (ileum) or the beginning of the large intestines. This happens when nutrients are moving too quickly (increased gastric motility, as in diarrheal illnesses) or simply too much food. The L-cells located in the ileum and colon will secrete GLP1 to slow down the movement of nutrients through the gut. This is the so-called ileal brake.
Administering GLP1 significantly slows down the movement of food through the intestines, slowing glucose release and telling us to stop eating.
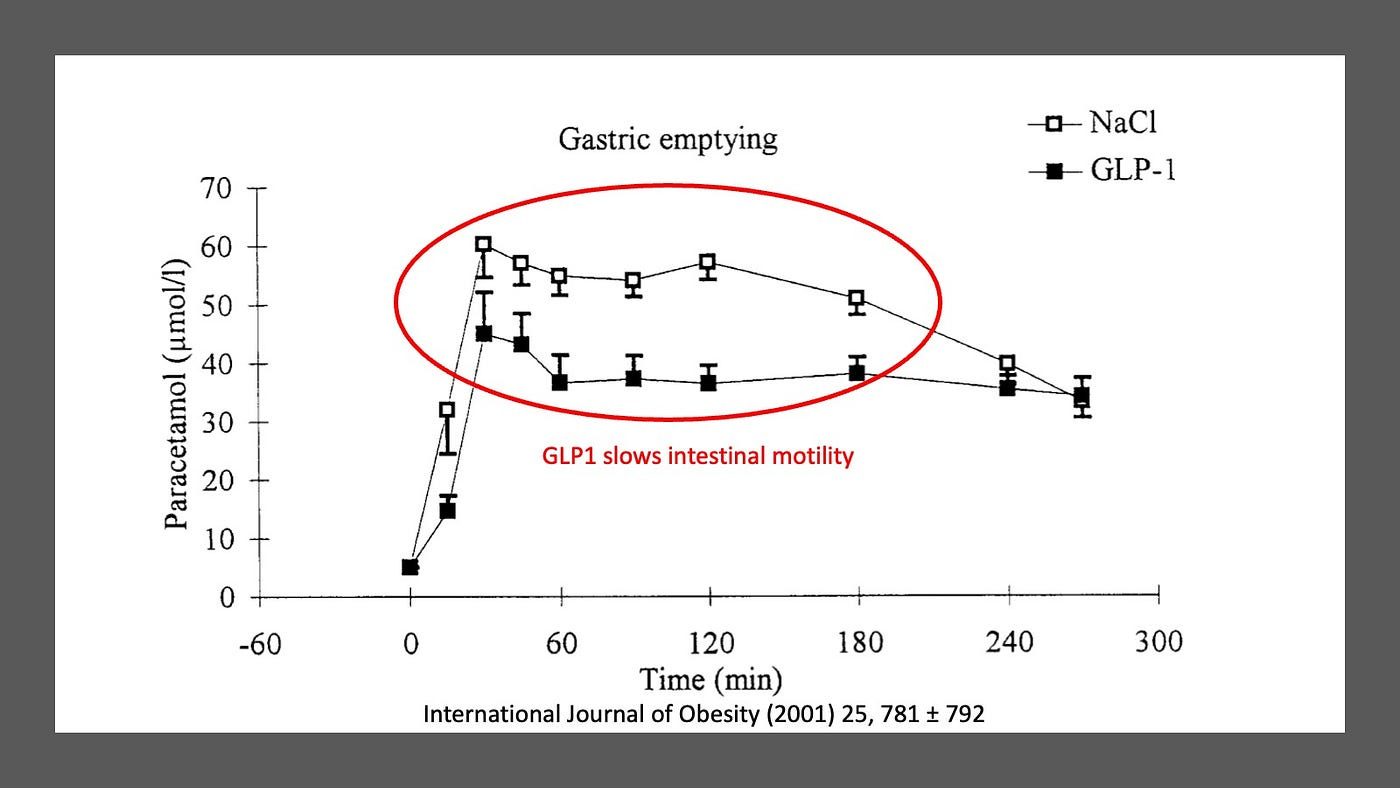
Incretins slow gastric emptying
Central Nervous System — control of appetite and weight
The effect of GLP1 on the control of appetite is likely the most important reason why drugs like Ozempic are effective.
People eat for many reasons, and not simply because your body needs nutrients. You may still be tempted to eat a donut or cookie even if you’re not hungry. Why? Because they are delicious — that is, you eat for pleasure. Discussing calories, or carbs, or macronutrients or protein or vitamins is pointless if the reason we are eating is for pleasure.
Highly palatable foods, typically high in refined carbohydrates and fat activate brain structures, such as the orbitofrontal cortex, insulin, amygdala and striatum. We experience “anticipatory food reward” and this is associated with increased cravings. Once you eat these food, dopaminergic neurons send connections to forebrain areas that results in a pleasant feeling, which is called cosummatory food reward.
It’s easy to see how this can result in overeating. Many things can release dopamine and give us pleasure. If we socially isolate ourselves, or stop doing things that give us pleasure, as happened during the recent pandemic, we may then seek to increase our dopamine by eating more. Taken to extreme, this can lead to addictive behaviors.
The area of the brain known as the hypothalamus main area controlling food intake. This includes the interconnected nuclei of the arcuate nucleus (ARC), paraventricular nucleus (PVN) and the dorso-medial nucleus (DMN). But how does the stomach and intestines send their signals to the brain? GLP1 is secreted by the intestinal cells into the peripheral blood and crosses the blood brain barrier at the circumventricular organs where the barrier is leaky. Once through, it can interact with receptors in the hypothalamus and area postrema to deliver its effects. In this way, GLP1 in the general circulation powerfully reduces appetite and therefore food intake.
Increased GLP1 signalling will reduce food cravings (decrease anticipatory food reward) and make us more full (increase cosummatory food reward) by influencing dopamine neurotransmission. This leads to reduced intake of hyper palatable foods which will generally lead to weight loss.
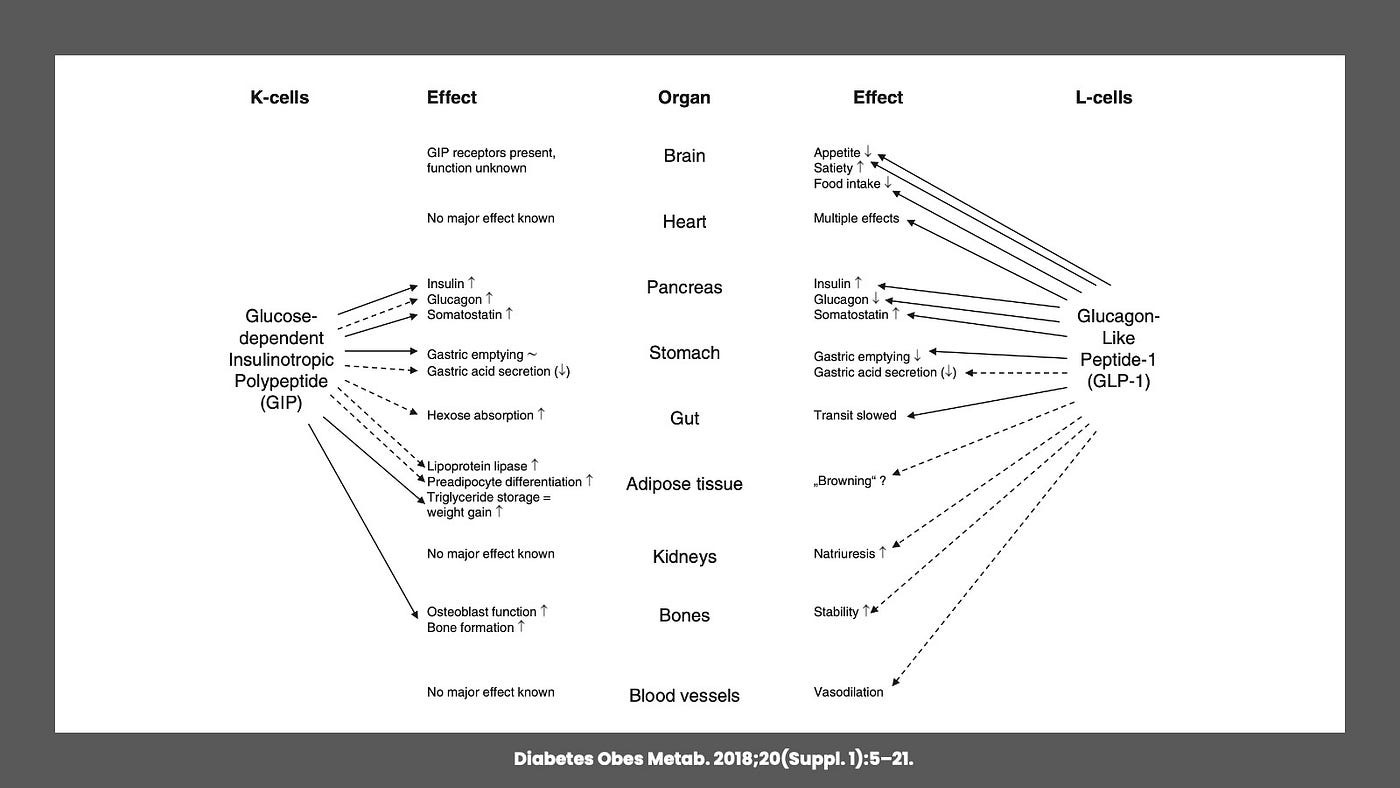
Multiple Effects of Incretins
The ARC contains two sets of nuclei — the orexigenic neuropeptide Y (NPY) and pro-opiomelanocortine (POMC), as well as cocaine and amphetamine-regulated transcript (CART) expressing neurons. When released, the POMC and CART activate hormones that inhibit food intake. Opposing this, DMN neurons activated by the NPY promote food intake. GLP1 receptors are highly expressed in the hypothalamus, but most in the POMC/CART neurons in the ARC.
Dietary Fat and GLP1
Dietary fat is mostly triglycerides — which are emulsified by bile acids, hydrolyzed by lipases, and then absorbed by enterocytes in the form of glycerol and free fatty acids. Free fatty acids are potent stimulators of GLP-1 release.
Different fats have different effects. For example, olive oil, compared to butter — stimulated more GLP1 release. A Mediterranean diet rich in olive oil decreased insulin and increased GLP1.
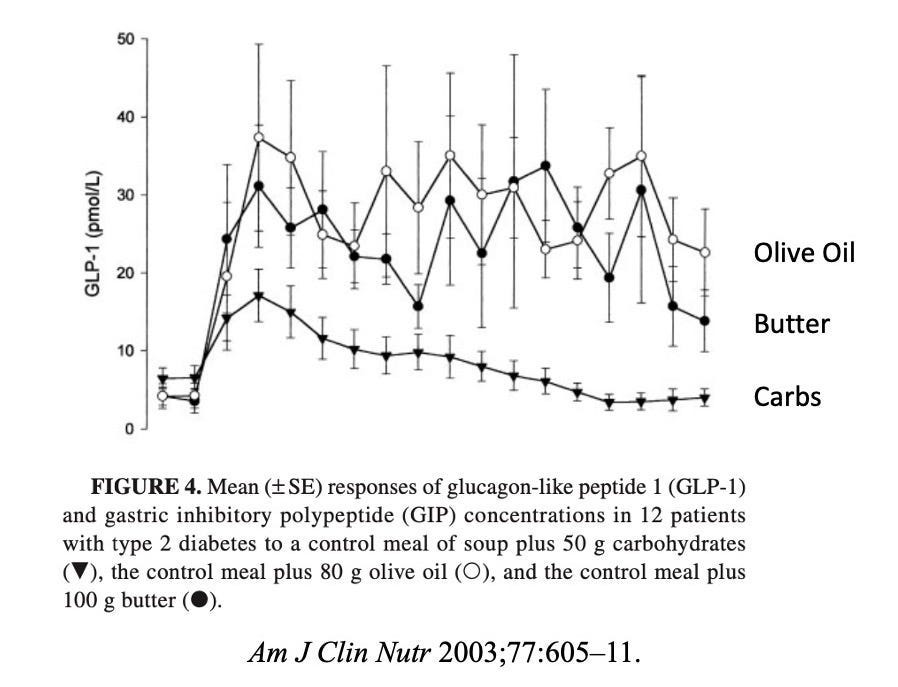
Dietary Fat increases incretins more than Carbs
In one study, test subjects with type 2 diabetes ate a control meal of soup with either carbs, olive oil or butter. The addition of carbohydrates had a lower peak GLP1 as well as a lower sustained level. The same held true for GIP.
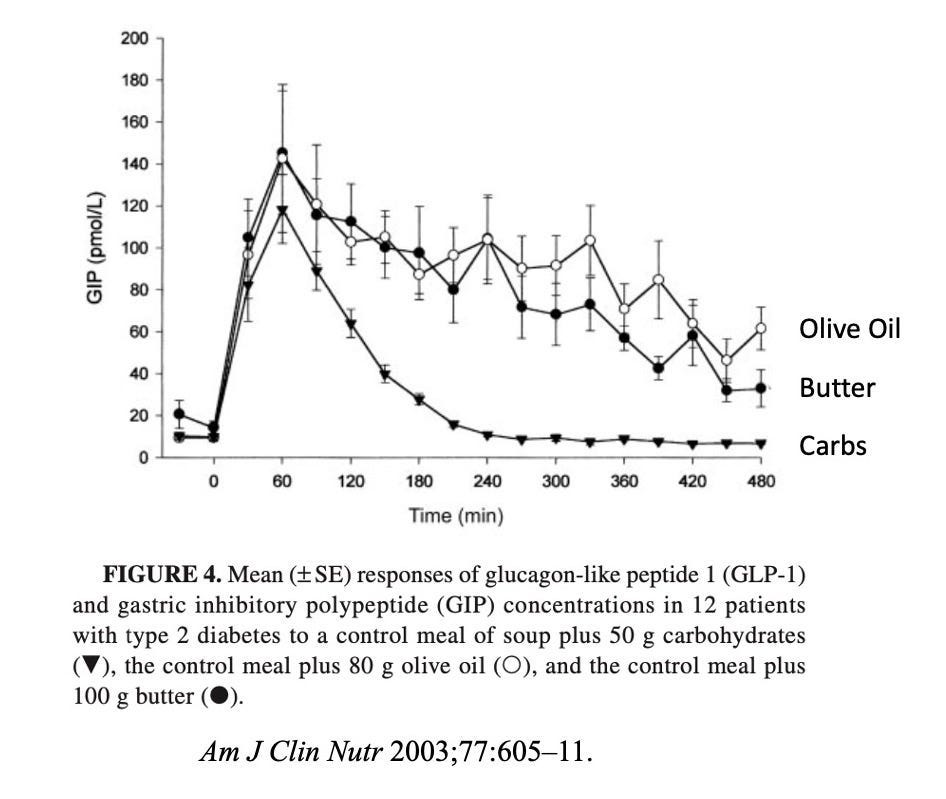
Dietary Fat also raises the incretin GIP more than Carbs
The practical implication is that substituting carbohydrates for fats leads to an increase in GLP1 and GIP, which helps increase satiety and reduce hunger. If you are less hungry, you will eat less in the future, which is conducive to weight loss.
Other studies showed much the same results. Insulin resistant patients were assigned to one of three diets — high carb (65% carb), high monounsaturated fat (think olive oil) and high saturated fat (think butter) for 28 days (still 47% carbs so not very low carb) and asked to eat the same calories.
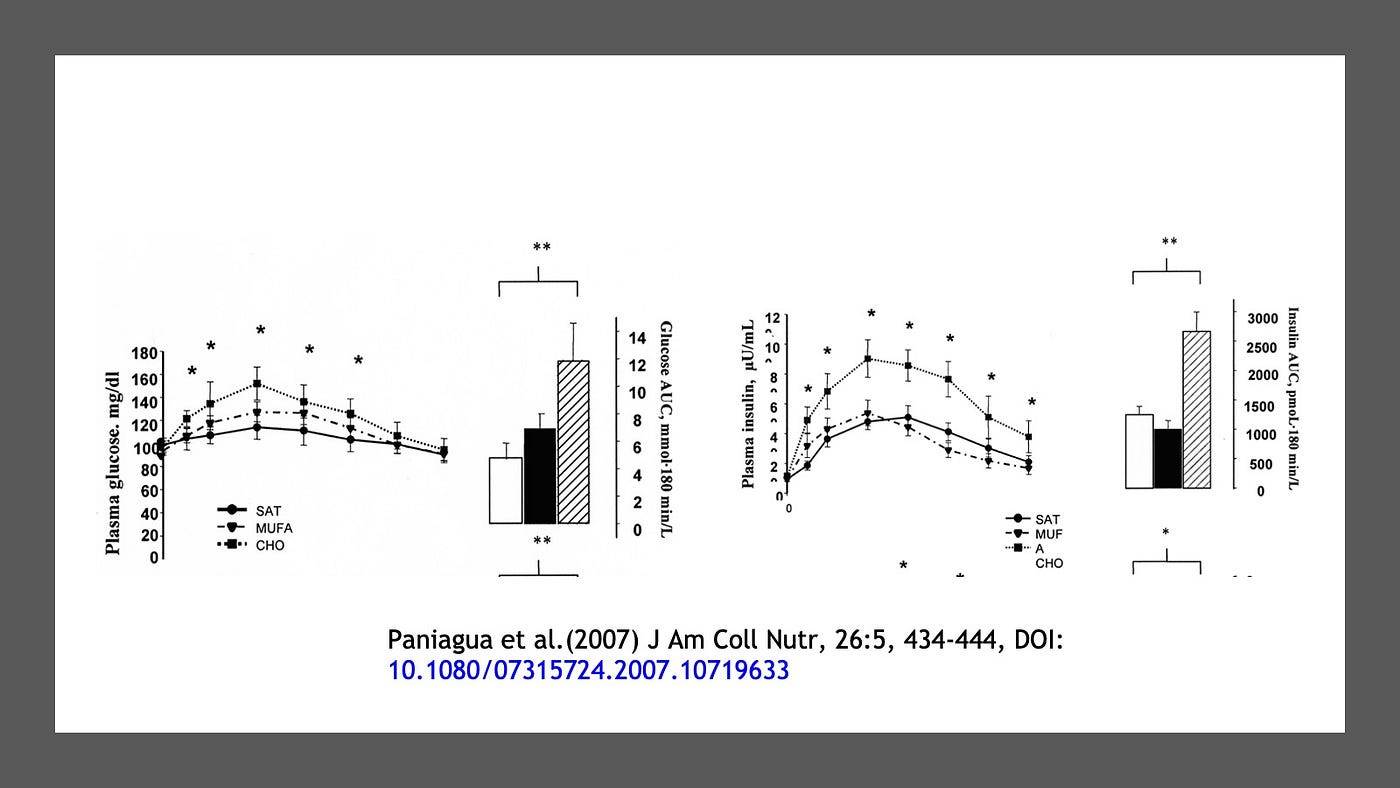
High Carb diets raise glucose and insulin more than lower carb
As expected, eating fewer carbs and more fat led to lower glucose and insulin levels. But what about the effect on GLP1?
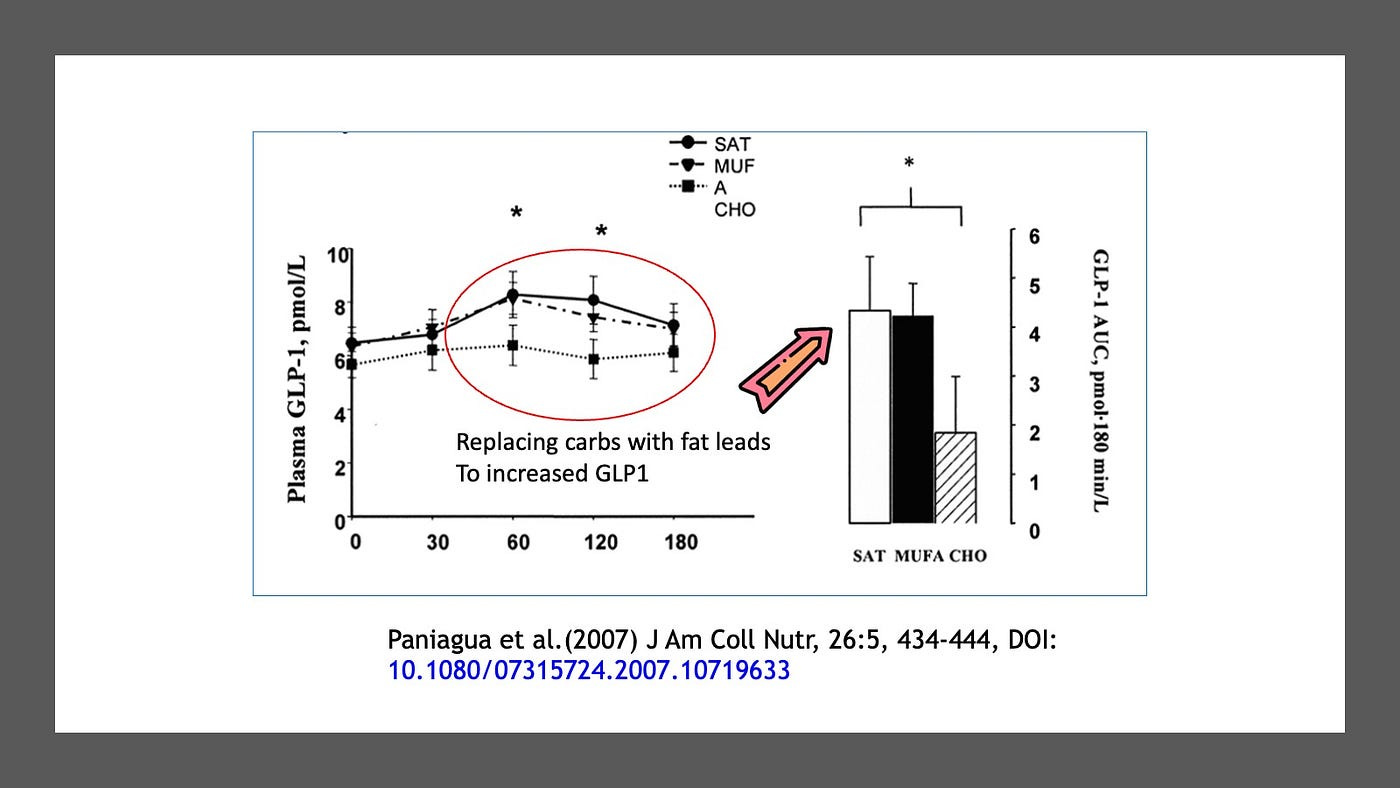
Higher fat diets raise GLP1
As in the previous study, eating fat (both saturated and unsaturated) instead of carbs, but keeping calories equal resulted in a significantly higher GLP1 level and area under the curve (AUC). Higher GLP1 equals feeling more full and therefore less likely to eat in the future.
Eating more fat doesn’t really lead to more heart disease. See my YouTube video on saturated fat for more.
Protein and GLP1
Protein tends to increase satiety more than an equivalent amount of dietary fat or carbohydrate. The mechanism behind this effect may be that higher protein diets increase GLP1 secretion which leads to less hunger.
One study compared a high protein (30%) diet to an adequate protein diet (10%), replacing protein with carbs and keeping dietary fat at 30%. The adequate protein diet is not a low protein diet, since it provided 1g/kg/day, which is still more than the Recommended Daily Allowance of 0.8 g/kg/day. For reference, the average American eats closer to 1.2 or 1.4 g/kg/day. Subjective hunger was measured with a visual scale and the high protein group was much less hungry after the meal (felt more full) and also before the next meal (felt full for longer).
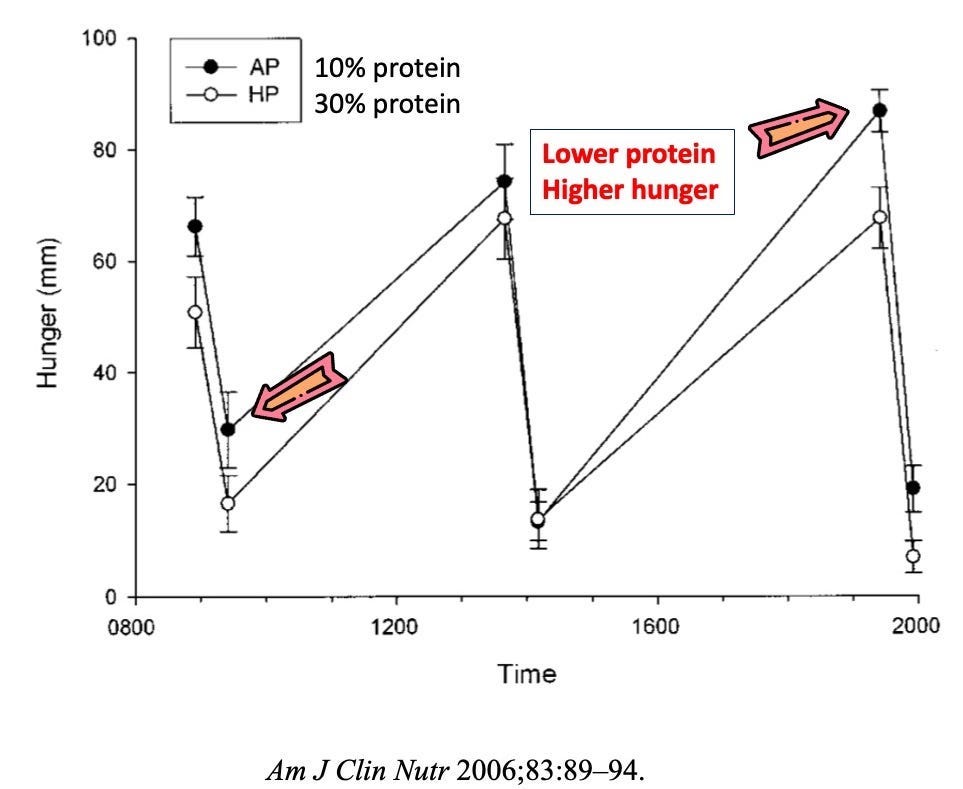
Higher Protein diets, Less Hunger
This effect may be related to the GLP1 effect of the dietary protein and is particularly noticeable at breakfast and dinner. The high protein breakfast included chicken breast and milk, compared to the adequate protein group of coconut bread and orange juice.
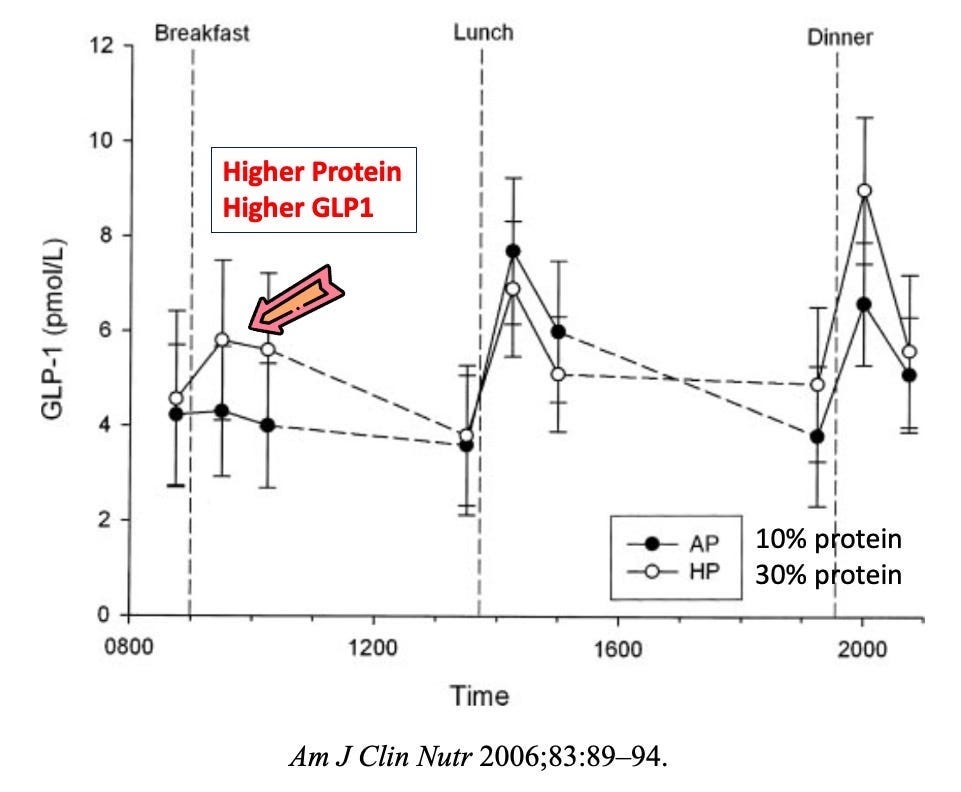
Higher Protein, Higher GLP1, Lower Hunger
The type of protein plays a role in GLP1 secretion as different amino acids have different effects. Branched chain amino acids, such as found in dairy products are particularly effective, as are caseins, often found in dairy. This reduces overall energy intake.
Protein also has the highest and most prolonged thermic effect of the macronutrients. This is the energy it takes to digest the food — for protein 20–30%, carbohydrate (5–15%) and fat (0–3%), which may explain an extra 50–150 calories per day increase in energy usage. Protein may also activate the sympathetic nervous system and this diet induced thermogenesis (DIT) may increase energy expenditure.
Other Dietary Considerations
Different carbohydrates can also have differing effects on the incretins. Fiber, a form of resistant starch can increase GLP1 secretion in the colon, where it ferments to SCFA (Short Chain Fatty Acid — acetate, butyrate, and proprionate). The SCFAs interact with free fatty acid receptors 2 and 3 to increase GLP secretion from L-cells. Diets high in resistant starch also increased Peptide YY secretions from the L-cells, a hormone known to increase satiety.
Experimentally, the targeted delivery of proprionate to the colon was enough to cause experimental subjects reduced subsequent food intake and over time , caused weight loss.
Bitter foods (bitter melon, bitter gourd) have been traditionally used in type 2 diabetes and this effect may be mediated through GLP1. For example, bitter gourd increases GLP1 through bitter taste receptors which may contribute to its anti-diabetic actions. Curcurmin may also stimulate GLP-1 secretion through activation of calmodulin-dependent kinase II.

Bitter Gourd
Practical Considerations
Losing weight, as I’ve noted before, is not so much about controlling the calories, but about controlling the hunger. We eat more when we are hungry, so the root cause of ‘overeating’ may be ‘over-hunger’. You can control how much you eat directly, but you can’t control how hungry you are. To do so, you must understand what is going to alleviate hunger, and the incretins GLP1 and GIP are key hormones to understand. (Also see this article about Fasting and Weight Loss)
Note that GLP1 agonists produce supra physiologic levels of GLP1. The DPP4 class of medications merely sustain physiologic levels and are not associated with very much weight loss. Therefore, the physiologic actions that promote GLP1 release are likely insufficient to cause the same degree of weight loss compared to the agoinst drugs (eg. Ozempic).
Replacing carbohydrates, specifically the highly refined carbohydrates with either protein or fat is likely to increase GLP1 secretion which makes us more full, and prolongs this feeling of fullness. This, naturally is conducive to weight loss. (See video — How to Lose Weight for more)
Dr. Jason Fung

Online Fasting Community and Coaching
For more, check out my YouTube channel, online community and coaching programs at TheFastingMethod.com and my Website & Books
Probably the most actionable and enlightening post so far. So easy to see the mechanism of the cosummatory desire for specific foods and the levels of food addiction. How it is like and unlike nicotine addiction for example. You can wash nicotine out of the system in two weeks and the psychological desire becomes easy to conquer. For the food addicted, washing the picture of the offending desired foods is harder.
The effects of the GLP-1 and GIP that will naturally occur and can be enhanced are real.
Most can relate to the loss of appetite that will eventually occur when either fasting or
dieting correctly (as described in this post). It takes longer than two weeks-likely, but it
happens and at that point it's important not to mess it up, which seems for many where the
mis-step happens.
You are one of the best go-tos for diet related issues.